When measuring heart attack risk, one important red flag is often overlooked, doctors say

[ad_1]
Heart disease kills more people in the U.S. than any other cause of death — yet many Americans aren’t aware of one major genetic risk factor.
Lipoprotein(a), or Lp(a), is a protein that can greatly increase the chances of a heart attack when it’s present in high levels in the blood.
Fox News Digital spoke with Dr. Seth Baum, a cardiologist and chief scientific officer at Flourish Research in Boca Raton, Florida, about the importance of this often overlooked red flag.
COLORADO CARDIAC NURSE, AFTER THREE HEART ATTACKS, OFFERS SURVIVAL TIPS: ‘LISTEN TO YOUR GUT’
What is Lp(a)?
Along with low-density lipoprotein (LDL) and high-density lipoprotein (HDL), Lp(a) carries cholesterol through the blood.
The higher your levels of Lp(a), the more likely that cholesterol will build up in your blood vessels, increasing the risk of a heart attack or stroke.

Heart disease kills more people in the U.S. than any other cause of death — killing one person every 33 seconds. (iStock)
“Lp(A) contains a particle that leads to cardiovascular disease when it’s in higher concentrations,” Baum said.
There are three main elements of Lp(A) that put people at risk, the cardiologist said.
REDUCING SALT INTAKE BY JUST 1 TEASPOON A DAY HAS SAME EFFECT AS BLOOD PRESSURE MEDS, STUDY FINDS
The first is that it causes atherosclerosis, which is the buildup of fats and cholesterol in the arteries.
“Another is that it causes inflammation, which is a really important aspect of plaque progression and the risk of creating a heart attack,” Baum said.
The third component, which is also vital in the genesis of a heart attack or a stroke, is that Lp(a) increases the risk of clotting, the doctor said — which could block off the artery.
“We call it a triple threat,” Baum said.
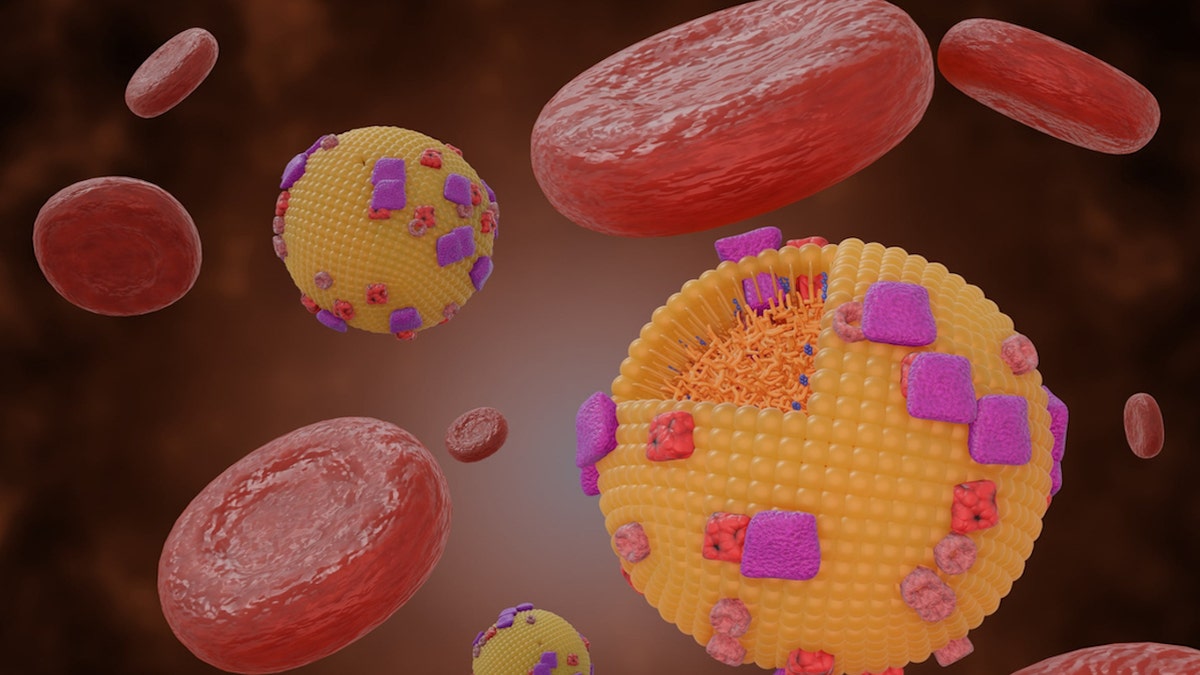
Along with low-density lipoprotein (LDL) and high-density lipoprotein (HDL), Lipoprotein(a) carries cholesterol through the blood. (iStock)
Brett Sealove, M.D., chief of cardiology at Jersey Shore University Medical Center, agreed that Lp(a) is an indicator of a serious threat.
“These ‘bad cholesterols’ result in plaque build-up in the arteries and reduced blood flow to vital organs, including the brain, heart, kidneys and legs,” he told Fox News Digital.
“The evidence is irrefutable — Lp(a) is considered an independent risk factor in addition to classic heart disease risk factors.”
Who is at risk?
Approximately 20% of the population is at risk because of Lp(a).
“These are very, very big numbers,” Baum said. “And it’s even higher than that in certain genetic groups.”
STANDING AND EVEN SLEEPING ARE BETTER FOR YOUR HEART THAN SITTING, NEW STUDY SUGGESTS
Black and South Asian Americans are at particularly high risk.
Despite that high prevalence, only a negligible share of Americans know their Lp(a) levels, the doctor pointed out.
“Probably fewer than 1% of the population has had their Lp(a) levels checked,” he estimated.

The higher your levels of Lp(a), the more likely that cholesterol will build up in your blood vessels, increasing the risk of a heart attack or stroke. (iStock)
Dr. Bradley Serwer, a cardiologist and chief medical officer at VitalSolution, a Cincinnati, Ohio-based company that offers cardiovascular and anesthesiology services to hospitals nationwide, noted that the cost and limited access to Lp(a) testing can be a problem.
“When trying to assess heart health risk, we often use risk screening tools that estimate an individual’s 10-year risk for developing significant cardiovascular disease,” he told Fox News Digital.
DOES THE FLU INCREASE THE RISK OF HEART ATTACKS?
“These calculators take into consideration age, gender, blood pressure, cholesterol levels and smoking history — but they do not include Lp(a),” he went on.
“Since these nationally accepted tools do not include the lipoprotein(a) in their score calculation, some insurance companies do not cover the cost of the testing.”
What can be done?
While LDL is genetically driven in a small subset of the population, Baum said, that type of lipoprotein is heavily influenced by diet and exercise.
Lp(A), however, cannot be controlled by lifestyle factors.
“There’s no therapeutic currently available that will reduce Lp(a),” Baum said.
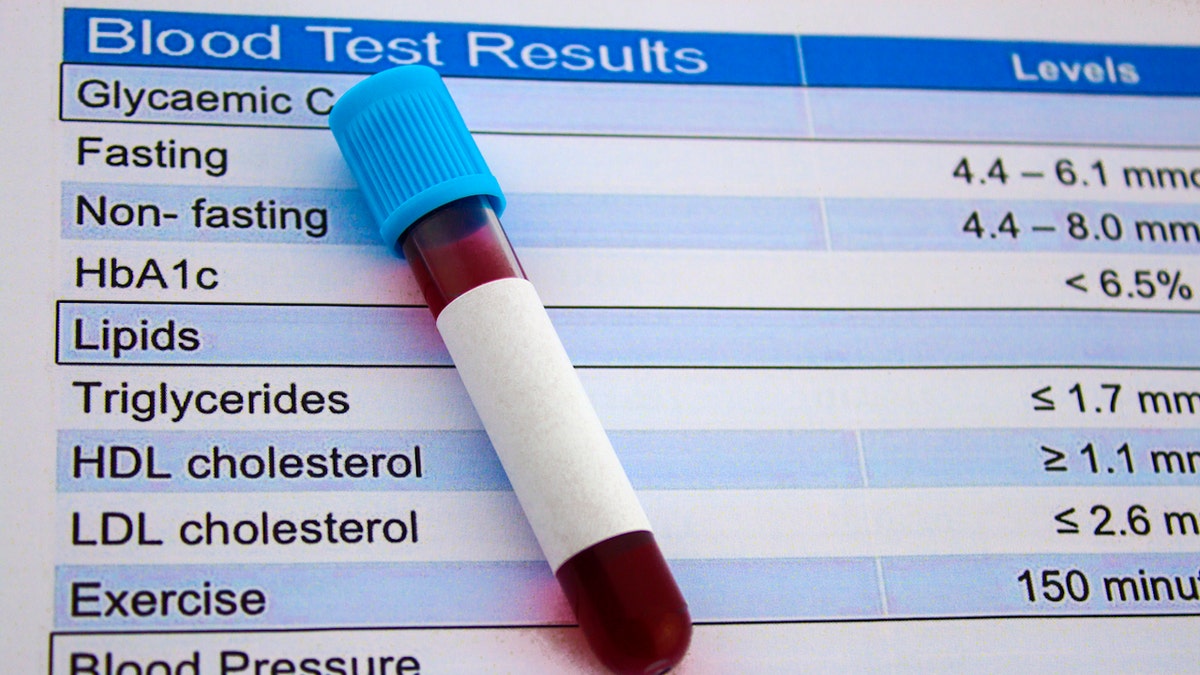
Lp(A) levels can be tested through a simple blood sample. (iStock)
So why check the levels if there’s nothing that can be done?
“Even though we can’t directly reduce Lp(a), we can reduce other cardiovascular risk factors,” Baum said. “You’ll still have the Lp(a) risk, but you won’t have all the other stuff floating around — so you can mitigate some of the overall risk.”
In Europe and Canada, the doctor noted, there are guidelines in place that state everyone should have universal screening for Lp(a) levels.
WANT TO LIVE LONGER? FOLLOW 8 HEART-HEALTHY HABITS, SAYS THE AMERICAN HEART ASSOCIATION
“In America, we’re a little behind the times — we still only check Lp(a) in patients who are at a higher risk,” he said.
Some doctors, like Baum, recommend testing Lp(a) levels for everyone, with the idea that if patients know they are more susceptible to heart attacks, they will be much more likely to reduce other cardiovascular risks.
Lp(A) levels can be tested through a simple blood sample.

At a minimum, Baum recommends getting Lp(a) levels checked at least once, and then again in the event of certain health changes. (iStock)
The levels tend to be relatively stable throughout the patient’s lifetime, the doctor said, but some elements can shift the Lp(a) a little in either direction.
“For example, going through menopause can dramatically increase Lp(a) levels, as can low thyroid or kidney disease,” Baum noted.
At a minimum, the doctor recommends getting Lp(a) levels checked at least once, and then again in the event of certain health changes.
“Probably fewer than 1% of the population has had their Lp(a) levels checked.”
Sealove agreed that patients should have their Lp(a) checked at least once as a screening test — “especially for those with a family history of heart disease and in conjunction with other laboratory parameters, including the standard lipid panel and other metabolic tests.”
In Serwer’s opinion, the decision of whether to test Lp(a) levels is a personal one that should be discussed with a medical provider.
“Before any medical test is ordered, it is important to know what you’re going to do with that information,” he told Fox News Digital.
Researchers are working to better understand Lp(a) and its role in diagnosis, risk assessment and potential therapeutics. (iStock)
“If knowing the Lp(a) level will make a difference or alter medical decisions, then it may be beneficial to measure.”
Regardless of the Lp(a) level, Serwer strongly recommends reducing cardiovascular risk factors with lifestyle, diet and exercise.
“The best way to combat atherosclerotic disease is to avoid it entirely — and the best way to do that is to start a healthy lifestyle as early as possible.”
Future of Lp(a) therapy
There is one therapy, called lipoprotein apheresis, that involves removing Lp(a) from the blood using IVs.
“It’s a technique we use to basically cleanse the blood of bad lipoprotein,” Baum said.
There are some drugs in development to treat high Lp(a).
Baum has a lipoprotein apheresis center in South Florida, and there are more than 40 other centers around the country.
This therapy is only available to a small number of patients, however.
CLICK HERE TO SIGN UP FOR OUR HEALTH NEWSLETTER
“We pretty much limit these for people who are very, very high risk,” Baum noted.
There are some drugs in development to treat high Lp(a), said Baum, who is heavily involved in clinical research.
“Those of us who know about these studies are very excited, because there is a real possibility that we’re going to do something significant in the not-too-distant future — that we’re going to have a therapeutic drug to reduce the risk of elevated Lp(a),” Baum said.

Regardless of the Lp(a) level, Serwer strongly recommends reducing cardiovascular risk factors with lifestyle, diet and exercise. (iStock)
Sealove reiterated that researchers are working to better understand Lp(a) and its role in diagnosis, risk assessment and potential therapeutics.
“Currently, several clinical trials are underway that target Lp(a), with more long-term outcome trials to come,” he told Fox News Digital.
CLICK HERE TO GET THE FOX NEWS APP
“Until these treatments become available, patients and doctors should focus on optimizing traditional risk factors and educating themselves about the impact of Lp(a) on cardiovascular health.”
For more Health articles, visit www.foxnews.com/health.
[ad_2]